Summary
Triangular Fibrocartilage Complex (TFCC) Injuries, a common cause of ulnar-sided wrist pain, may result from trauma or due to degenerative changes.
Diagnosis is made clinically with ulnar sided wrist pain that is worse with ulnar deviation and a positive « fovea » sign. An MRI can help confirm diagnosis.
Treatment is generally conservative with NSAIDs and immobilization. Surgical debridement, TFCC repair or ulnar shortening procedures may be indicated depending on severity of symptoms and underlying cause.
Anatomy
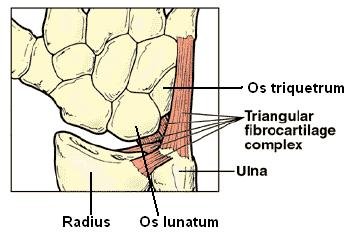
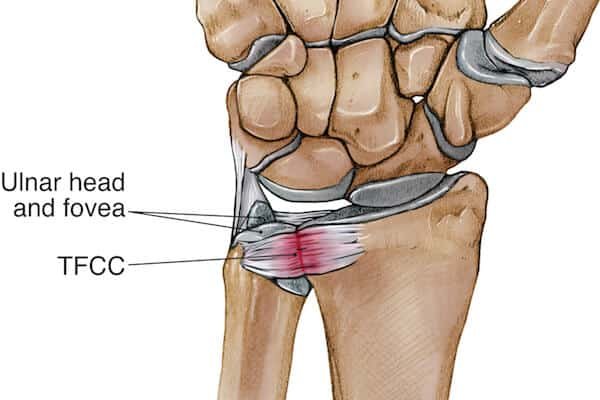
TFCC made up of dorsal and volar radioulnar ligaments deep lig, known as ligamentum subcruentum, attach to the ulnar fovea
superficial fibers attach to the ulnar styloid central articular disc
meniscus homolog ulnar collateral ligament ECU subsheath
origin of ulnolunate and ulnotriquetral ligaments
Blood supply
periphery is well vascularized (10-40% of the periphery) central portion is avascular
Origin
dorsal and volar radioulnar ligaments originate at the sigmoid notch of the radius
Insertion
dorsal and volar radioulnar ligaments converge at the base of the ulnar styloid deep fibers insert on to the ulnar fovea superficial fibers insert on the ulnar styloid
Case
A 33 year old male patient presented to the outpatient with pain left wrist since one year. He mentioned he had a fracture of the distal radius that was operated in another hospital. The fracture healed but now he feels pain on pronosupination and tenderness over TFCC.
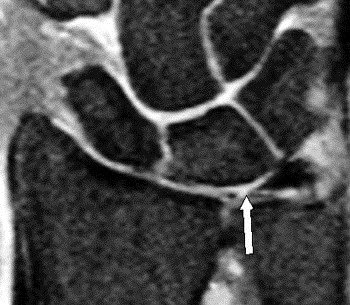
MRI left wrist ordered:
report: subchondral cysts and bone edema on distal ulna. Small subchondral cyst in the triquetrum bon. TFCC: Mild thickening at the ulna styloid attachment and small central partial tear. Tendons : Edema of the extensor carpi ulnaris tendon. Mild effusion at the dorsal aspect of the radio-ulnar joint and in the pisiforme-triquetrum joint.
- Surgery was indicated: ulnar diaphyseal shortening surgery
- indication :Type II with ulnar positive variance is > 2mm
advantage of effectively tightening the ulnocarpal ligaments and is favored when LT instability is present
Below are x rays before and after surgery
Post Surgery the patient recovered well and had no pain on pronosupination as before surgery